Creating a Patient Monitoring System
Scalable digital solution connecting hypertensive patients and nursing teams in a managed care environment.
Context
Medicinia
Health-tech startup focused on safe, human-centered communication between healthcare companies, physicians and patients.
MOPE
Special Patient Monitoring Team (MOPE in Portuguese). Nursing team dedicated to remotely monitoring patients from the health insurance company São Cristóvão Saúde (based in Brazil).
Problem
Business Problem
The MOPE Team needed to increase patient coverage without increasing nurse workload or clinical risk using a digital solution as a way to expand and enhance its reach, capacity and quality of care.
Business Need
Align product scope with clinical constraints, operational capacity, and measurable outcomes for remote hypertension programs.
User Problem
Nurses needed workflows that reduced cognitive load during remote follow-ups while keeping patients engaged between in-person visits.
User Need
Clear, timely communication channels and lightweight tasks patients could complete without friction on common devices.
Why was this important?
As patient volume increased, the monitoring team could not scale manual follow-ups without compromising care quality and nurse workload.
Goal
Design a digital monitoring system to scale patient coverage without increasing nurse workload or clinical risk, while giving patients a structured way to maintain daily health routines between follow-ups.
Research & Insights
Understanding the problem
To understand the context, exploratory conversations were conducted with the monitoring team (team leaders, nurses, and attendants) to learn how patient monitoring was currently performed, the challenges faced, and unmet needs.
For patient context, the MOPE team helped to select patients that could be part of the pilot solution.
Research
Research focused on understanding existing monitoring workflows, patient engagement, tracked health indicators, data organization, and communication during follow-up. In parallel, we reviewed the hypertension care protocol to identify the key events and indicators that would guide the solution.
Key Insights
Informal tools created coordination risk. Nurses managed patient communication through WhatsApp and spreadsheets. There was no unified view of patient status and no reliable way to flag what required immediate attention.
Not all indicators carry the same urgency. Blood pressure readings require a different response speed than monthly weight tracking or quarterly appointments. A single undifferentiated flow could not serve all of them safely.
Patients needed structure, not just access. Without reminders and contextual guidance, daily adherence depended on patient initiative alone. Routine-building had to be designed into the system, not assumed.
Key Outcomes
Clinically relevant indicators:
- Quarterly consultation with a specialist
- Semiannual consultation with a second specialist
- Daily blood pressure control
- Daily medication control
- Monthly weight control
MOPE team's current processes
- Patient communication managed through informal channels
- No unified view of patient status
- No structured way to flag urgent readings
- Care coordination dependent on individual nurse initiative
From Insights to Design Decisions
Interviews revealed informal workarounds and unclear prioritization. The protocol defined indicators and thresholds, pointing toward a modular, indicator-specific system with direct communication channels.
Solution
The solution was structured around a core insight from research: different health indicators require different monitoring logic. Rather than a single linear flow, the system was designed as a modular architecture where each indicator defines its own communication channel, frequency, and response behavior.
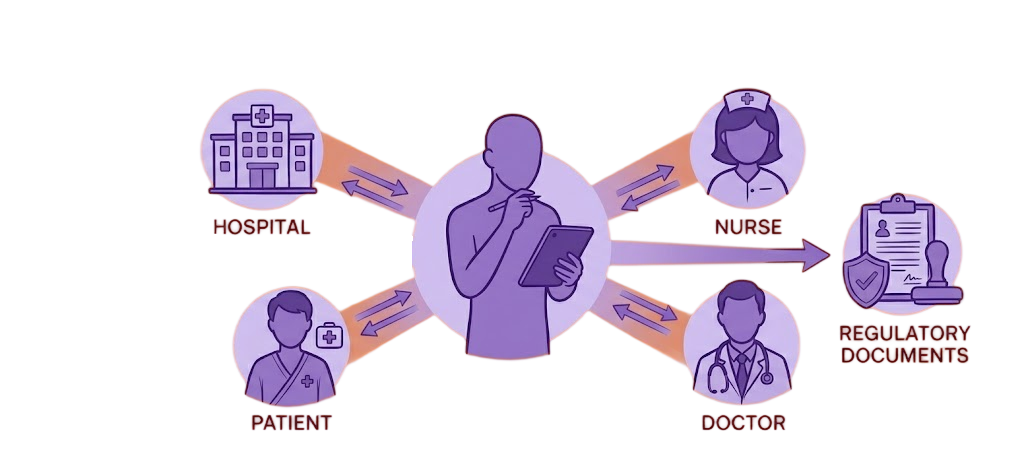
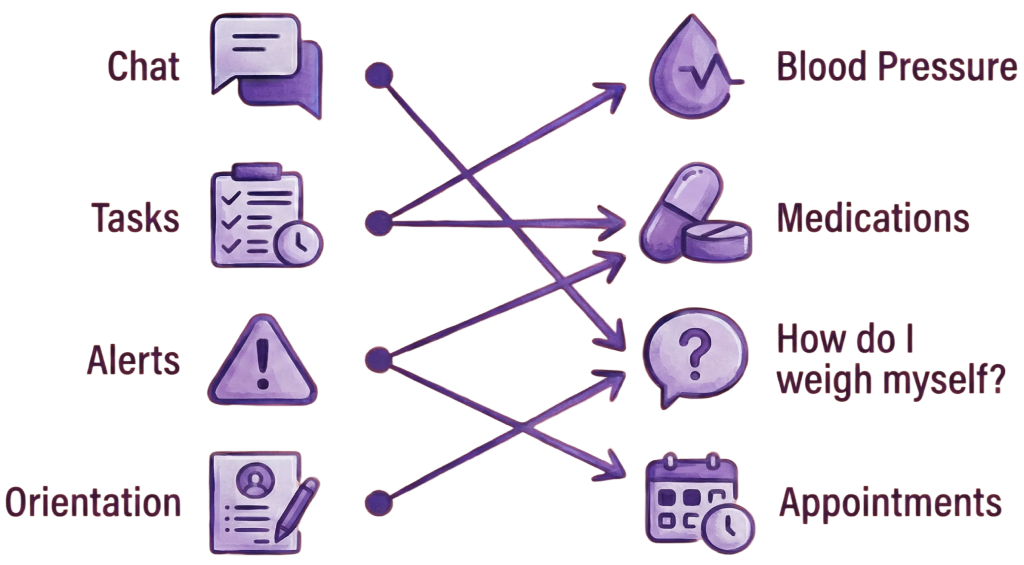
Defining Contact Channels by Indicator Context
Based on each indicator’s type, relevance, and frequency, different patient contact channels were defined for each monitoring context. This ensured that health data was exchanged through the most appropriate channel, giving nurses and the system the right conditions to act on what patients reported.
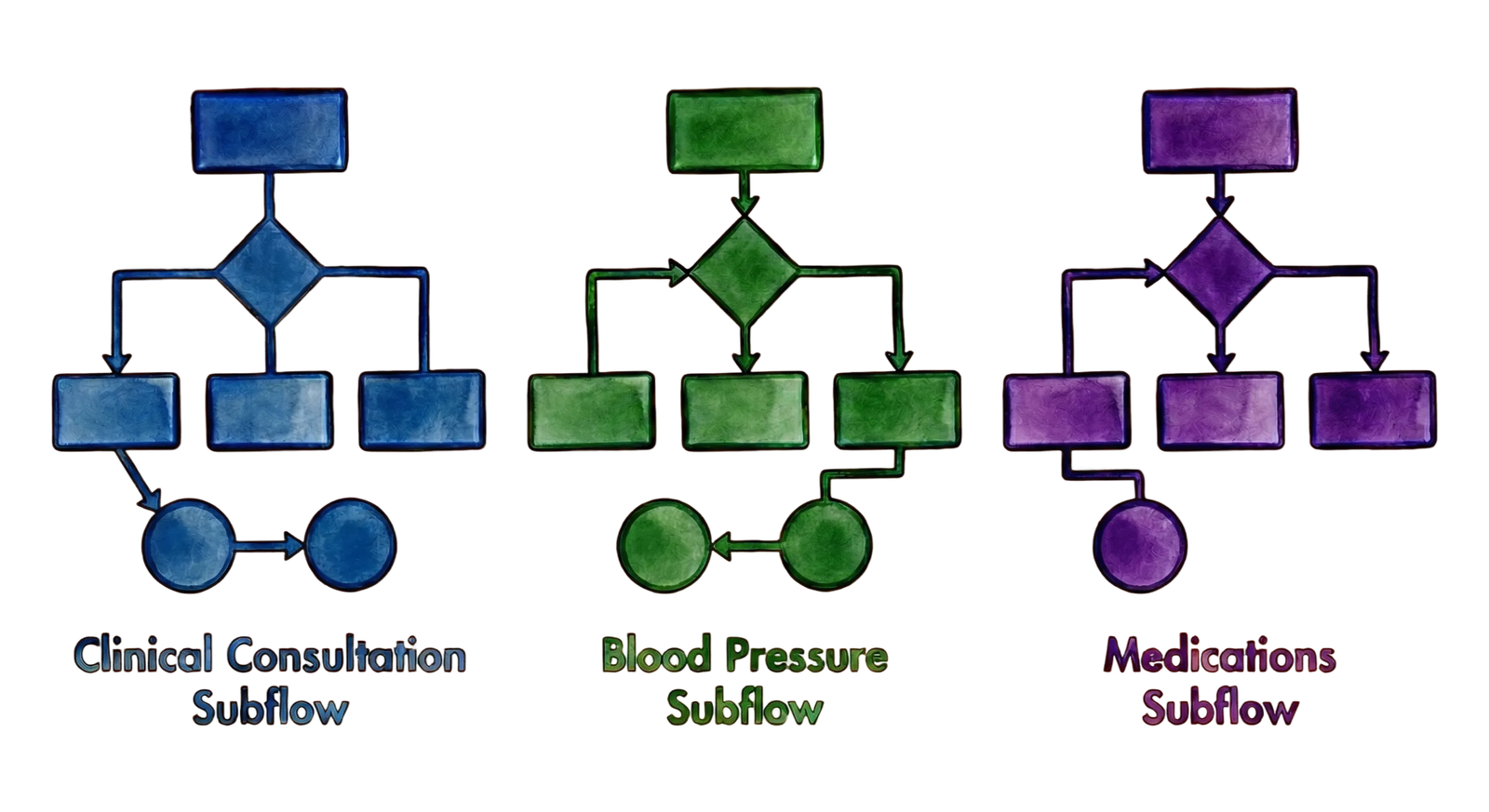
Patient Tracking - Overview
Patient monitoring was structured as a set of independent subflows, each designed around a specific indicator’s clinical urgency, measurement frequency, and the patient’s ease of interaction. Together, all subflows form the complete monitoring architecture.
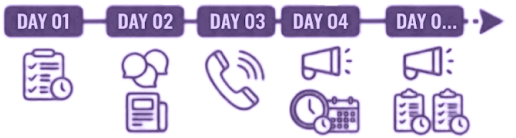
Progressive Patient Onboarding
With multiple indicators and explanations to introduce, onboarding was deliberately spread across the first week of app use. Each task and orientation was delivered only when contextually relevant, reducing early friction and improving long-term adherence.
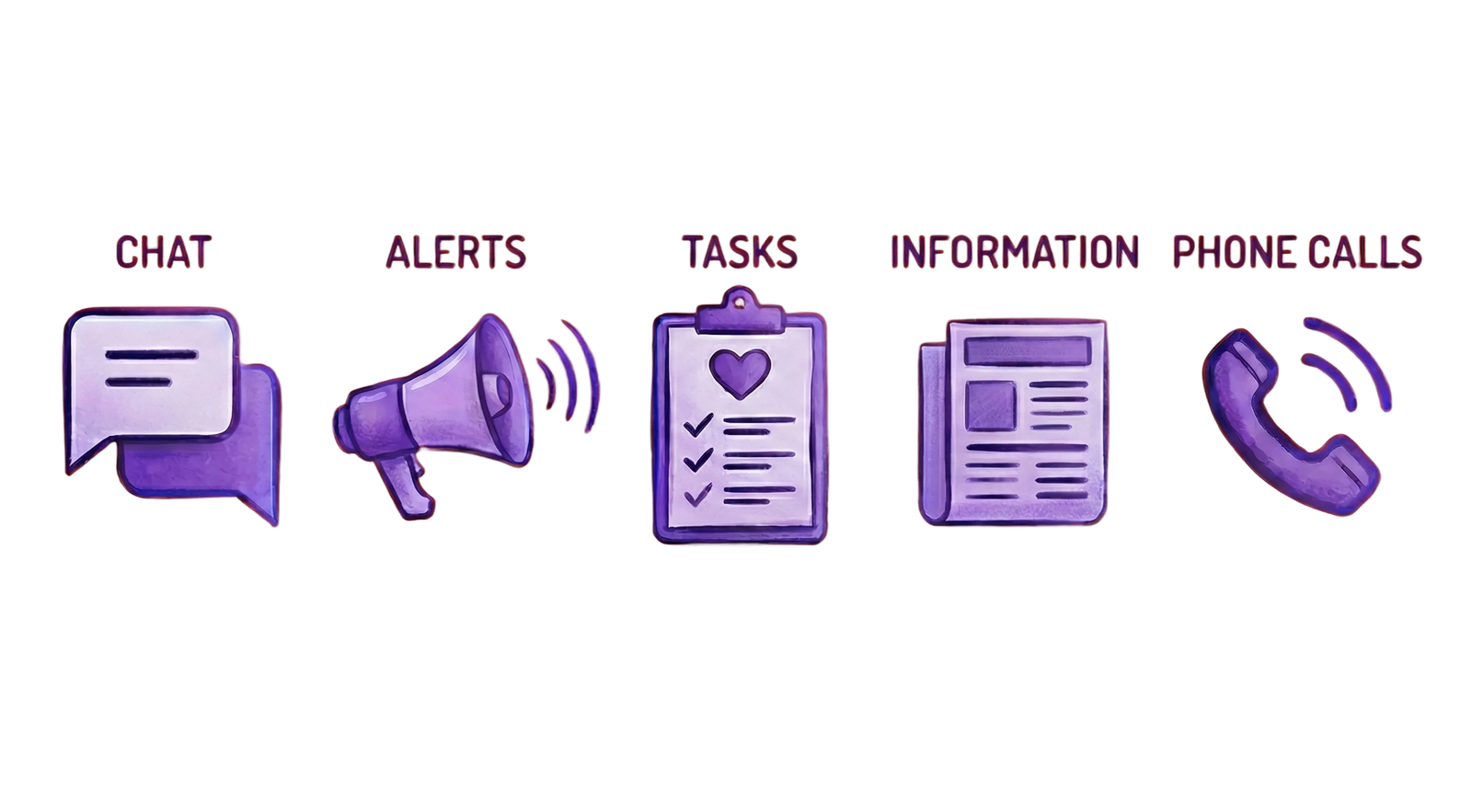
Channels x Indicators
Each health indicator was mapped to the most appropriate contact channel based on its urgency, frequency, and content type, forming the modular foundation of the monitoring system.
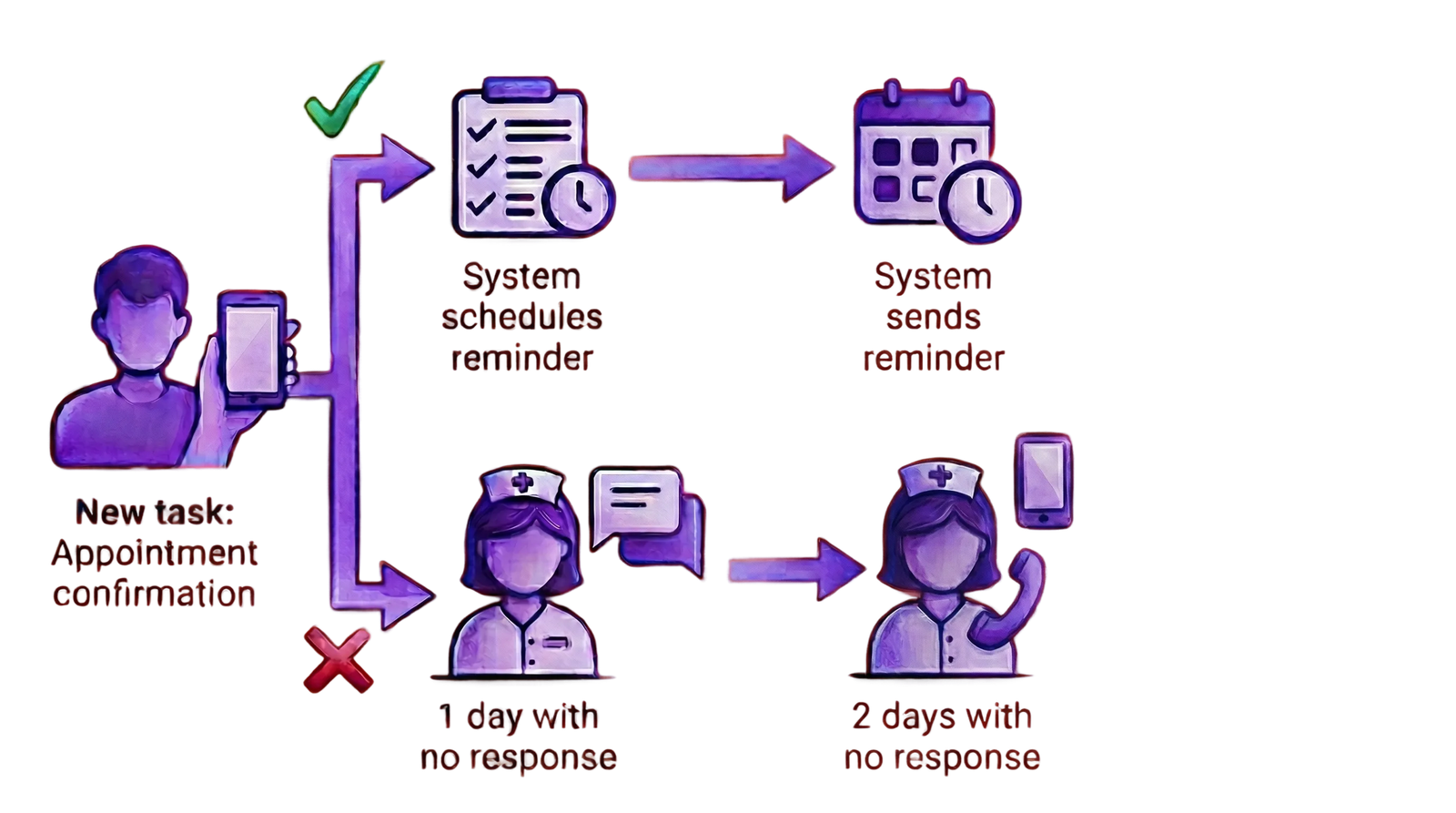
A Subflow in Practice
The appointment confirmation sub-flow illustrates this logic: if a patient confirms, the system schedules a reminder automatically. If there is no response, escalation triggers nurse intervention after defined time thresholds.
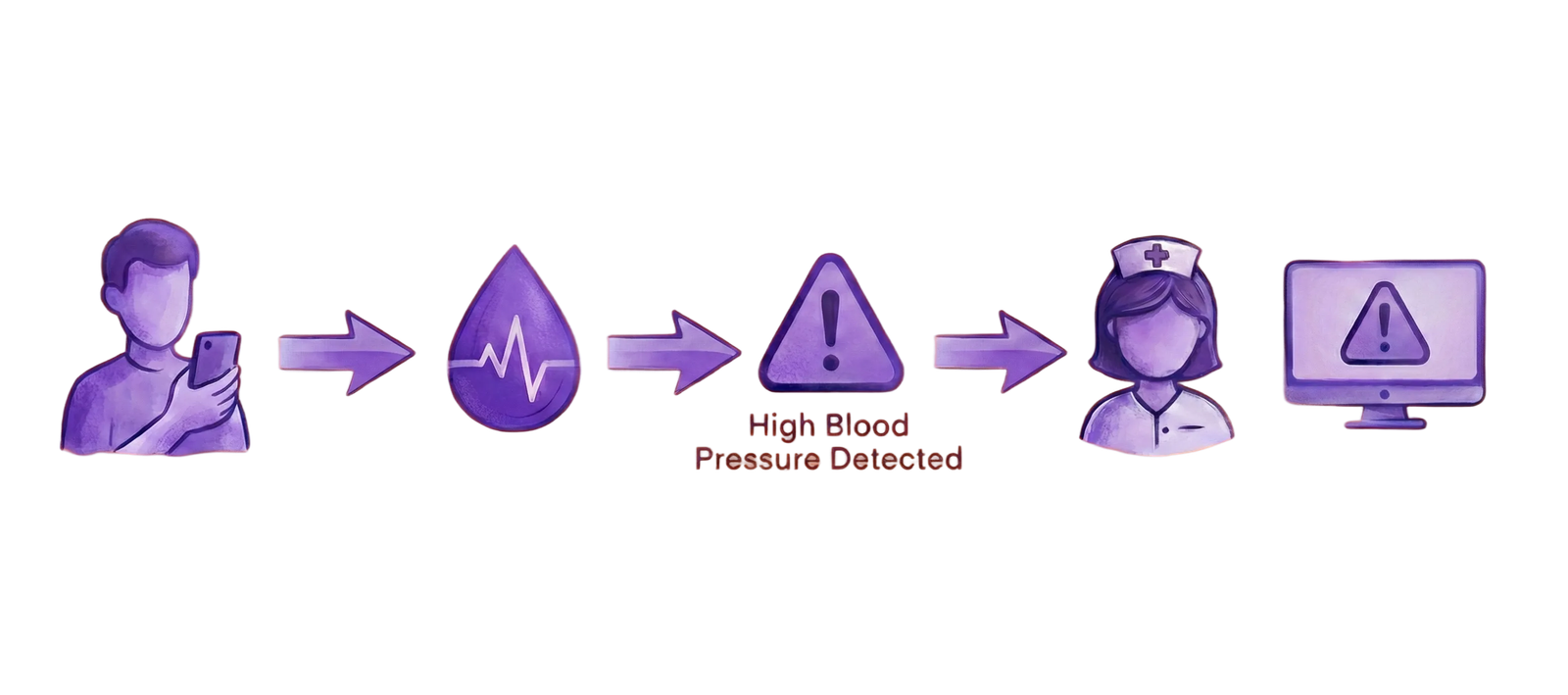
Designing for Fast Clinical Response
Nurses needed immediate visibility into patient-entered data and timely alerts when readings crossed clinical thresholds. I advocated for contextual triggers that gave the monitoring team a clear, objective view of each patient throughout the monitoring period, enabling faster risk recognition and appropriate response.
Translating Architecture into Tangible Design
With the monitoring logic, communication channels, and interaction points between nurses and patients defined, the work moved into translating these decisions into user flows and low-fidelity interfaces.
Key Strategic Decisions
Accelerating learning through Web View
To maximize learning speed during early validation, patient-facing screens were implemented using Web Views instead of native components. This decision significantly reduced deployment friction, allowing the team to iterate on UX, content, and interaction patterns without repeated app store releases and enabling faster response to insights from testing.
Designing for change with a flexible backend
I collaborated closely on the definition of the backend data model, advocating for a generic and extensible structure. This approach allowed indicators, flows, and clinical protocols to evolve over time without major structural changes, supporting both scalability and long-term product adaptability.
Validating workflows before automation
Rather than automating processes prematurely, early testing relied on manual triggering of tasks and alerts, with the monitoring team acting as test patients. This deliberate choice prioritized understanding real workflows and refining UX and system logic before committing to automation, reducing downstream rework and risk.
Modeling for evolution
Advocating for a generic backend model involved close collaboration with engineering to balance short-term delivery pressure with long-term flexibility.
The indicator-based flow model established a reusable foundation that could support additional conditions beyond hypertension without redesigning the system.
Summary
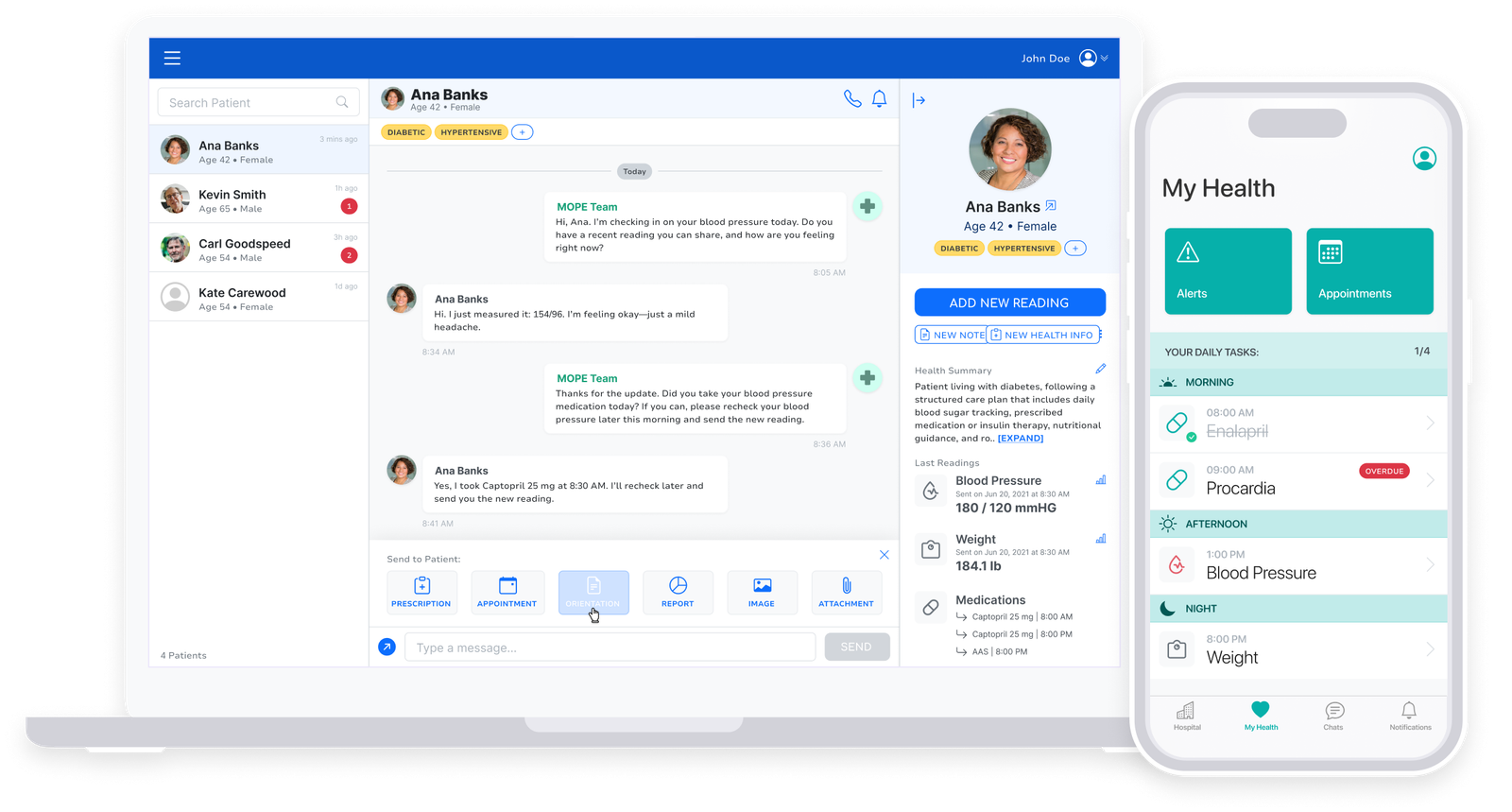
Two complementary surfaces
Indicator-specific subflows connect these two components through patient data entry and system events. Together, automated responses and nurse interpretation form a unified monitoring flow that supports continuous, safe patient follow-up.
Accelerating learning through embedded web view
The solution can be understood as two complementary components:
- Tools for the monitoring team including:
- Chat,
- Alerts for critical indicators (such as abnormal blood pressure or weight), and
- Easy access to patient data.
- A patient-facing app with chat, tasks, alerts, reminders, and educational content to support daily monitoring.
Outcomes & Learnings
Outcomes
- Delivered a modular monitoring MVP aligned with clinical protocols and real nurse workflows.
- Enabled safe scaling by combining automated alerts with nurse interpretation instead of a single linear process.
- Improved patient comprehension and adherence through progressive onboarding and contextual communication.
- Provided nurses with a unified view of patient communication and recent indicators, reducing cognitive load during follow-up.
Key Learnings
- Adherence depends on timing, not volume: distributing indicators and guidance over time reduced friction and confusion.
- Clinical monitoring requires modularity: decoupling channels and content allowed each indicator to define its own flow.
- Automation supports (but does not replace) clinical judgment: alerts were most effective when paired with context and human analysis.
- Healthcare UX is systems design: small interaction decisions can significantly impact safety, workload, and trust.